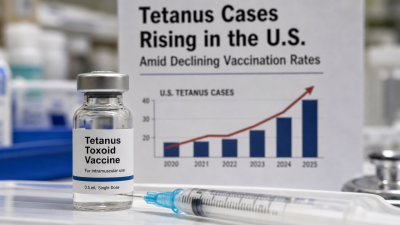
Tetanus cases in the United States rose to 38 in 2025, the highest annual count since 2006, occurring alongside declines in childhood DTaP/Tdap vaccination coverage.
Etiology & clinical features
- Clostridium tetani: spore-forming anaerobe; produces tetanospasmin neurotoxin.
- Neurotoxin blocks inhibitory neurotransmitters causing trismus (lockjaw), generalized muscle spasms, dysphagia, autonomic dysfunction and seizures.
- Recent US case-fatality ~12%; mortality concentrated in older adults.
Epidemiology — recent data
- 38 confirmed cases in 2025; 32 cases in 2024 (CDC reports).
- Four paediatric cases in 2024 (Idaho, Minnesota, Missouri, Wisconsin); all unvaccinated; some declined post‑exposure prophylaxis.
- Kindergarten DTaP coverage fell to 92% (2024–25) from ~95% a decade earlier; declines reported in over 75% of US counties.
- Florida: state DTaP 88.8% (2024–25); Broward County 82.2%.
Vaccination, prevention & post‑exposure care
- Vaccine: DTaP five‑dose childhood series; Tdap/Td boosters every 10 years.
- Pregnancy: single dose of Tdap recommended each pregnancy (27–36 weeks) to protect neonates.
- Post‑exposure management: wound care, human tetanus immune globulin (TIG) when indicated, and vaccine booster if due.
IASPOINT Booster Facts
- CDC conducts national surveillance and issues guidance on tetanus prevention and post‑exposure prophylaxis.
- WHO elimination objective applies to maternal and neonatal tetanus via maternal immunisation and clean birth practices.