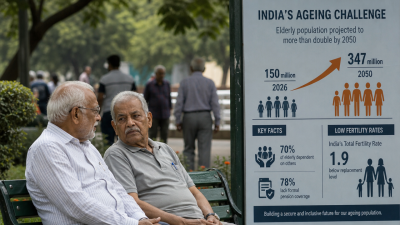
India’s fertility has fallen below replacement. National TFR is 1.9; urban fertility about 1.5. Several states record ultra‑low TFR (1.2–1.3) while poorer states retain higher fertility. The elderly population is 150 million and may reach 347 million by 2050, creating urgent demands on income support, health systems and labour markets.
What is the issue and why it matters
Current status
National TFR: 1.9 children per woman. Urban TFR: ~1.5. Spatial divergence: Delhi 1.2; Kerala, Tamil Nadu, West Bengal 1.3; Bihar 2.9; Uttar Pradesh 2.6; Madhya Pradesh 2.4; Rajasthan 2.3. Elderly (60+) currently ~150 million, projected ~347 million by 2050. Reports show high economic vulnerability among the elderly and low pension coverage.
Why it matters for governance and economy
- Public finance: Rising pension and health expenditures amid an unconsolidated tax base and incomplete industrialisation.
- Labour markets: Long‑term risk of labour shortages in low‑fertility states and regional mismatches.
- Social support: Families can no longer be the sole safety net as old‑age dependency grows.
- Health systems: Increased demand for geriatric, chronic and long‑term care services.
Distribution and patterns
| Dimension | Detail |
|---|---|
| National TFR | 1.9 children per woman |
| Urban–rural gap | Urban ~1.5; rural closer to replacement |
| Ultra‑low fertility states | Delhi (1.2); Kerala, Tamil Nadu, West Bengal (1.3) |
| High‑fertility states | Bihar (2.9); Uttar Pradesh (2.6); MP (2.4); Rajasthan (2.3) |
| Elderly population | 150 million now; projected 347 million by 2050 |
| Pension coverage | ~78% of elderly lack formal pension; ~70% depend on others |
Implications
Socio‑economic
- Dependency shifts: Lower child dependency but rising old‑age dependency increases care needs and household outlays for health.
- Family structures: Smaller families reduce intra‑family insurance and informal caregiving capacity.
- Consumption and savings: Ageing can change aggregate demand patterns and national saving rates.
- Gender and labour force: Opportunities to raise female labour participation, but also need for childcare and eldercare supports.
Health and care
- Geriatric care demand: More chronic disease, disability and long‑term care; need to integrate geriatric services into primary healthcare.
- Workforce needs: Train community health workers, geriatric specialists and long‑term care staff.
Governance and policy challenges
- Limited social security: Current schemes (Atal Pension Yojana, National Social Assistance Programme) provide partial coverage; informal workers remain largely outside formal pensions.
- Portability: Migrant workers need portable welfare and pension entitlements across states.
- Institutional readiness: India is ageing before completing industrialisation and before building broad tax bases or extensive welfare institutions seen in older economies.
- Service delivery: Primary health systems must adapt to chronic care models and geriatric services.
Economic and fiscal implications
- Fiscal pressure: Higher recurring expenditure on pensions and health will require either higher revenues or reallocation of budgets.
- Productivity risks: Smaller working cohorts in low‑fertility states can lower aggregate labour supply unless offset by productivity gains or migration.
- Policy levers: Widen the tax base, raise labour force participation (especially female), increase public investment in health and skill formation, and consider phased retirement or incentives to extend working lives.
Regional imbalances and federal response
Demographic divergence creates different policy priorities across states. Low‑fertility states will need services and old‑age incomes. High‑fertility states need jobs, education and skill formation for a large youth cohort.
- Migration and markets: Inter‑state migration can reallocate labour but requires portable entitlements and social protection.
- Cooperative federalism: Central incentives, conditional grants and fiscal transfers can balance investments in employment creation, health infrastructure and pensions.
- Data and planning: State‑level demographic projections must inform fiscal transfers, health provisioning and labour policies.
Policy options and instruments
| Policy | Objective | Expected outcome |
|---|---|---|
| Universal or broad contributory pension | Extend income security to informal sector | Reduce elderly dependence; predictable cash flows |
| Integrate geriatric care into primary health | Manage chronic disease and disability at scale | Lower hospitalisation, improve functional health |
| Portable social entitlements | Protect migrants and internal mobility | Labour market flexibility with social security |
| Active labour policies in high‑fertility states | Create jobs and skill youth | Positive demographic dividend; reduce distress migration |
| Fiscal reforms | Widen tax base; earmark funds for ageing needs | Sustainable funding for pensions and health |
| Urban and social infrastructure | Age‑friendly cities, eldercare services, affordable housing | Better quality of life; reduced familial burden |
Implementation priorities
- Phased approach: Scale social security and health reforms in phases, starting with poorest and most vulnerable elderly.
- Data systems: Strengthen civil registrations, pension registries and health records for targeting and portability.
- Inter‑sectoral planning: Align health, labour, finance and urban policies for coherent responses.
- Fiscal realism: Combine efficiency gains, targeted transfers and widened revenues to fund ageing commitments.
Model Questions
1. Analyse the socio‑economic implications of India’s rapid decline in fertility and the growth of its elderly population. How do these changes affect traditional family support systems and care arrangements? [GS-I: Indian Society]
India’s low fertility reduces future child cohorts and increases old‑age dependency. Households face higher care and health costs as family sizes shrink. Traditional intra‑family insurance weakens, raising demand for public pensions, long‑term care and community services. Labour dynamics shift: potential shortages in ageing states, altered savings and consumption patterns, and pressure to raise female labour participation. Policy response must combine income support, geriatric services and social care networks.
2. Evaluate the governance and policy challenges in preparing India for mass ageing before industrialisation and a widened tax base. What institutional reforms are required? [GS-II: Governance]
Challenges: limited pension coverage, weak geriatric care, non‑portable entitlements and constrained fiscal space. Reforms: broaden social security (contributory or universal pensions), integrate geriatric care in primary health, create national portability for welfare and pensions, strengthen fiscal transfers to states, and improve data systems. Institutional changes must prioritise implementation capacity at state and local levels and align incentives for cooperative federal planning.
3. Examine the economic and fiscal implications of India entering a phase of mass ageing. Suggest strategies to maintain economic stability and resource allocation for an ageing society. [GS-III: Economic Development]
Mass ageing raises recurrent pension and health expenditures and can compress the labour force, lowering potential growth. Fiscal strain emerges if revenues do not rise. Strategies: widen tax base, improve tax compliance, reallocate spending towards preventive health and care, raise labour force participation (women, older workers), invest in productivity and skilling, and design phased retirement or incentive structures to retain experienced workers while supporting young employment.
4. Discuss complexities arising from stark regional fertility differences in India. How can cooperative federalism address divergent needs of younger, high‑fertility states and older, low‑fertility states? [GS-II: Social Justice]
Regional divergence creates simultaneous needs: jobs and education in high‑fertility states; pensions, health and care in low‑fertility states. Cooperative federalism can use conditional grants, targeted central schemes, and fiscal transfers to align resources. Policies should promote inter‑state portability of welfare, incentivise job creation in younger states, and support state capacity building for eldercare. Data‑driven planning and shared funding mechanisms will balance demographic pressures fairly.
Last Modified: June 26, 2026